Bob
Parsons was 51 when he was diagnosed in
March 2002. His initial PSA was 46 ng/ml and his Gleason Score was 9. His journey
has taken many twists and turns as he has kicked and bucked against the way some
of his medical practitioners treated him and his diagnosis. Always curious about
this complex disease, in early 2011 he managed to view his original pathology
slides and get copies of them from a friendly pathologist. Here he shares what
he has learned.
I
had a renewed interest in pathology after a PCa seminar meeting - one of those
put on monthly by my local oncologist-doctor, who is just fabulous and after reading
about what German pathologist Dr.
Bonkhoff can do that other pathologists cannot or are not doing. My oncologist
answered my wishes after I told him I had read a seminar Journal article by Dr.
Bonkhoff which led to Dr Strum sending me a copy of a
joint paper [this is a large 3MB+ file]
that he and Dr Bonkhoff had written - and had given me permission to publish that.
Dr Strum was also kind enough to give me an indication of how the enhanced pathology
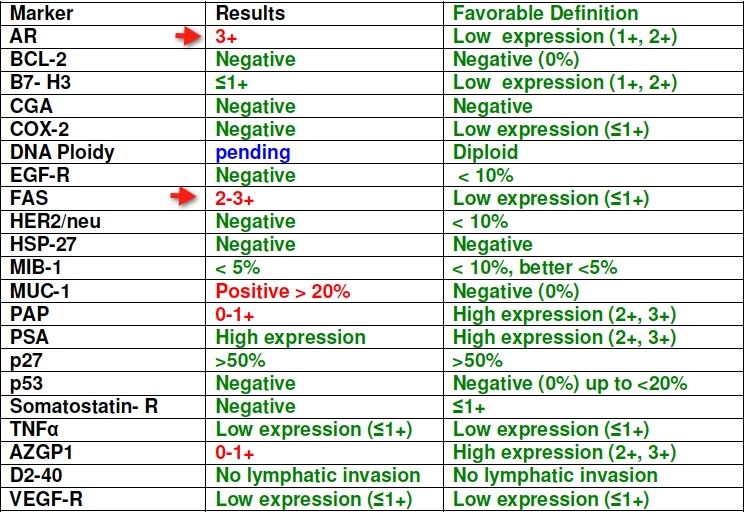
reports issued by Dr Bonkhoff are interpreted. Here is what the summary looks
like for a typical patient:
Using
this kind of analysis, it is possible to see what gene or enzyme is over expressed
or under expressed and make recommendations. For
example,
 If there were an over-expression (oE) of FAS (fatty acid synthase) then it might
be suggested that agents that can dR (down-regulate) FAS might be: Xenical (orlistat),
EGCG, 1,25 DHCC (Calcitriol), parasitic loranthus, GLA >alpha linolenic acid >
DHA;
If there were an over-expression (oE) of FAS (fatty acid synthase) then it might
be suggested that agents that can dR (down-regulate) FAS might be: Xenical (orlistat),
EGCG, 1,25 DHCC (Calcitriol), parasitic loranthus, GLA >alpha linolenic acid >
DHA;
On the other hand, if there were under-expression (uE) of p27, then: DHA, Silibinin,
beta-lapachone, calcitriol, magnolol (Honokiol), might be advised.
There
is a signficant problem in finding a local doctor who can actually interpret and
apply those details. Most men are fortunate if they can find a local urologist
who just keeps current on contents in one or two journals and is open minded enough
to honestly represent the several major treatment options. It is a sad commentary
on the urological community that this is so much of a challenge.
I
mentioned to my oncologist my objective of seeing my pathology slides, kept in
storage at Detroit Medical Center Hospital pathology laboratory and learning more.
He made it happen with a local hospital pathologist, a guy with 22 years experience
at pathology. He knew about Dr. Bostwick and some other renowned America pathologists
but had not come across Dr Bonkhoff and his work, so he had not seen the Journal
article. He did this for free as a favor to my oncologist-doctor and he did for
me, shows there are stand up people who give a darn.
I
had 12 biopsy shots. This gives six slides, some slides have four samples upon
them, your samples are often split, or cut somehow, down the middle and shown
as two sets (4) total to analyze. Regular chemistry slides are used, but also
a cover plastic sheet on top, to prevent scratching and docs says for better imaging
use.
The
Gleason Grading criteria changed in January 2011 and lowest graded known PCa is
now listed as Gleason Grade 3 using the normal combined grading system for samples
from needle biopsy procedures, thus Gleason 6 combined score is the lowest (3+3)=6.
No longer do we see or use Gleason combined scorings of 4, 5 or less (2+1)=3 and
such are defunct [See Gleason
Grades for more information].
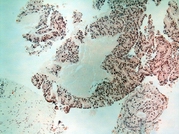
(click
for larger picture) | This
first photo is combined Gleason scores 9 (seen with photo is Gleason grade 5 and
maybe 4's also) On my pathological report A. and B. were Gleason 9's. See the
density of the red and dark red PCa cells, this is called cribiform pattern...mostly
consistent with Gleason grade 5 level. |
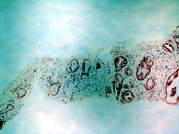
(Click
for larger picture) | Second
photo is likely my Gleason 7 graded samples, seeing large open tubular gland cells
(this more towards normal with open cells like this) |
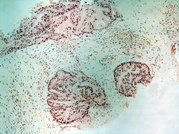
(Click
for larger picture) | Third
photo is more consistent with Gleason grade 4 patterns, and combined my scores
were in one sample (4+4)= Gleason 8 and another sample (3+5)= Gleason 8 The first
number in a combined Gleason scored is the more predominate graded PCa and then
follow by any secondary less volume percentage grade found. |
(Click
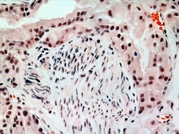
for larger picture) | Fourth
photo is enlargement at least 100X or more, the cells towards the center are curvey-
squiggly like in appearance...this is PNI (perineural invasion) it is surrounded
by the red looking PCa cells...thus the possibility of invasion into the blood
system, through this blood vessel/nerve. In PCa having PNI found on biopsies does
not mean it happened to travel, it is a prognostic risk factor and noted. People
have been cured of PCa and have even various samples found with PNI upon biopsies |
Some
of the other articles and papers I have read lately that deal with these pathological
issues are:
Targeted
therapy of cancer: new roles for pathologistsprostate cancer Mark A Rubin
A Proposal on the Identification, Histologic Reporting,
and Implications of Intraductal Prostatic Carcinoma [This
is a large - 3MB+ pdf file]
Ronald J. Cohen, MBBCH, FFPATH, FRCPA, PhD; Thomas M. Wheeler, MD; Helmut Bonkhoff,
MD; Mark A. Rubin,